

“Runner’s Knee”: How to Fix It and Keep Running Pain-Free

Did that picture of the person grabbing their bright red knee just slap you with an epiphany? Or maybe you are thinking “How did they get a picture of my knee in this book?” The image may have caused a form of PTSD and triggered your painful memories (literally). I am very sorry for the latter if it occurred, but we “knee-d” to discuss the cause and prevention of this dang thing!
Patellofemoral syndrome happens when the cartilage underneath the kneecap becomes irritated and inflamed. Our kneecap actually moves up and down (and a little side to side) within the grove of the thigh bone (femur) while we walk, run, bike, etc. This is due to the pulley mechanism of the quadricep tendon (above the patella) and the patellar tendon (below the patella). As the knee moves through flexion and extension, the tendons transmit forces while the patella places the muscles at optimum angles for muscular contraction. The patella is the fulcrum, essentially. If we did not have kneecaps, our muscles/tendons would sit too close to the actual knee joint and the muscles would have to work harder to move our limbs leading to more compressive forces at the joint and quicker/worse structural breakdown.

Can you imagine if that tiny little rock wasn’t sitting underneath the lever? Good luck trying to lift the stone off the ground without it.
Research attempts to measure the exact amount of compressive forces that act through the patella with different activities. Here is a table for my visual learners out there (holllaaaa):

Don’t be too alarmed by the numbers, but instead gain an appreciation for the difference in force between walking and running, or biking and running, even going down stairs vs going up stairs. These numbers were generated on healthy knees when the patella sits perfectly in its groove, is protected by a layer of articular cartilage, and has enough fluid to lubricate it while it moves along the joint surfaces. However, in the case of Patellofemoral Syndrome, we see a lack of patellar stability from weak and/or tight soft tissue structures normally responsible for the alignment and stability of the patella. This includes the quadriceps, adductors, VMO (a quad muscle), biceps femoris (hamstring muscle) and the ol’ ITBand (1). If even just one of those structures is tight, it pulls the patella out of its groove and creates increased compression and shearing forces along the bony surfaces of the femur.
Let’s be real - we are not suffering with just ONE of those structures being tight/dysfunctional. Typically, we are overly dominant AND tight in one of them. Or should I say, FOUR of them: The quads. Since the patella functions to enhance the force generation of the quad, the quads have the most power to influence its position and function. Patellofemoral Syndrome is diagnosed when our patella is shearing across bony structures it shouldn’t be in contact with during movement; thus, leading to articular cartilage damage and unwanted bony contact. Unwanted bony contact + repetitive motion = pain, grinding, curse words, swelling, etc.
How Does Runner’s Knee Happen?
As is true for most running injuries, this is typically due to overuse, overtraining, and bad repetitive motion over a long time. However, an acute bout of patellar tendonitis or patellofemoral syndrome can occur with trauma to the kneecap and surrounding structures (i.e. fall, collison). We will touch on both of these starting with trauma as this will be a short and sweet explanation.
Patellofemoral Syndrome can occur with direct trauma to the kneecap from a fall or collision such as tripping over a metal bar and bracing the fall with your kneecap smashing into another metal bar conveniently placed nearby. In this story, you are running a 50K and you are trying to run over one of those cattle bridge things next to the gate, which you could have gone through instead, but didn’t because you are racing and that would take time. This happened to a very good friend of mine, and her knee grew three sizes that day my friends. Her patellar tendon and kneecap were not happy, but survived and healed with rest, ice, KT-tape, and dry needling. Sometimes direct trauma can lead to worse injuries like a fractured patella or meniscus damage. Moral of the story - if your knee slowly inflates like a balloon and changes colors within 24-48 hours, then seek medical attention and do not run. Thank you. End of explanation on patellar injuries by direct trauma. Short yes, sweet - not so much.
Now let’s talk about bad, icky, non-glutey repetitive motions with poor mechanics causing sore and sharp knee pain. Y'all know what I’m talking about.
Our patella is shaped like a rock you’d find on the beach and want to skip across the ocean. It has some ridges, but is mostly smooth and flat. It has an edge that is rounded and an edge that is pointed.

The patella is also a puzzle piece fitting perfectly within the notch of the femur (thigh bone) and held in place by ligaments, tendons, and muscles. This notch (and the back of the patella) is lined with articular cartilage to make motion smooth and slidey (technical term).
“Poor patellar tracking” is a phrase commonly used with the diagnosis of Patellofemoral Syndrome to explain that the patella has been taken out of its little notch and asked to move along surfaces not intended for patellar contact.
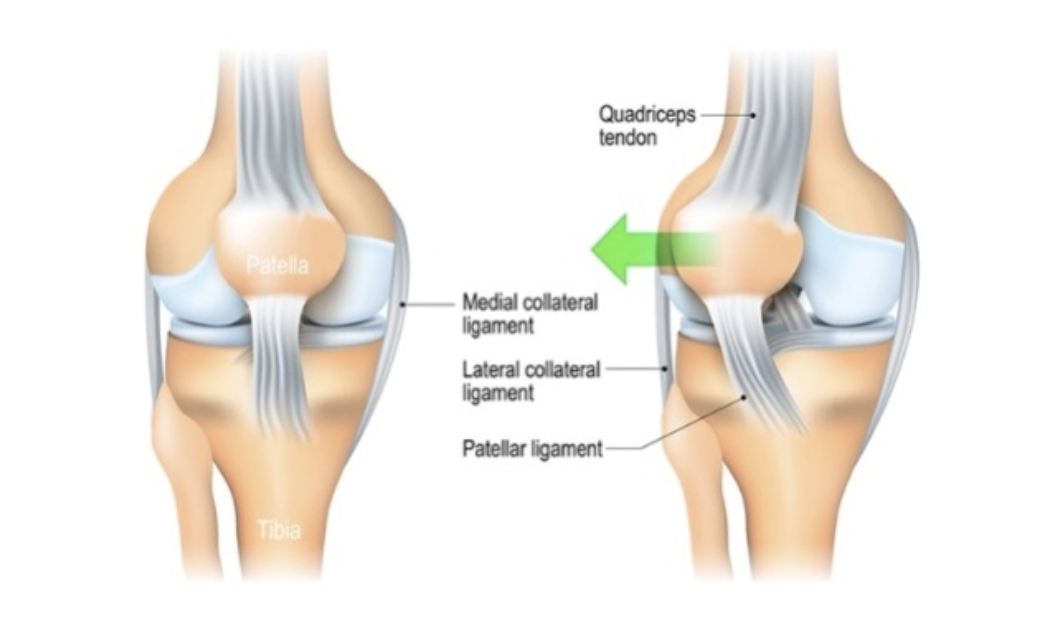
The patella is more commonly pulled out of alignment laterally (outside) and superiorly (upward) by tightness in the quadriceps tendon, muscles, “and ITBand.” Quotes in this case represent a statement that is still up for debate amongst clinicians and researchers. However, the alignment can also be altered by an excessive rotation of the femur/knee joint internally because the three gluteal bears are not activating to maintain proper knee alignment in single leg stance. This mal-alignment might be fine in a sedentary position; however, we have to move at some point, which means the patella will need to take on an amount of force (sometimes 2-3x bodyweight!!) soon. Excessive force + poor alignment = disaster.
For example, try to balance a pencil horizontally on top of your pointer finger. Find the spot in which the pencil is balanced evenly upon the fulcrum (your finger). You may also pinch the pencil at this spot with your thumb and pointer finger, wiggle it gently up and down, and find that it turns to rubber. This is a wild phenomenon worth exploring. However, back to fulcrum. Once it is balanced perfectly on the pad of your finger, I want you to pull the pencil a few millimeters in one direction and let go. Did the pencil fall to the floor? Shoot. Gravit: 1; Your pencil: 0. Pulling the pencil out of its perfect alignment lead to failure as the force of gravity was too much for the pencil to sustain. I suppose you could have bent your finger or twisted your hand in a weird way to help fight the force of gravity and keep the pencil from falling - but that would feel uncomfortable and you probably wouldn’t do that.
But wait, our patella doesn’t just fight against gravity, it also has to deal with ground reaction forces and muscles forces acted upon it. This pencil metaphor isn’t exactly the same.
BRILLIANT! You learn fast, young grasshopper. Let’s explore this further.
There is the analogy that our bodies are like vehicles - needing proper alignment, fuel, and maintenance to keep things running smoothly. Have you ever experienced your car or tires being out of alignment? You might feel the wheel shaking, bumpy car rides, the car pulling in one direction, or fighting the steering wheel to keep it straight. This can happen from hitting a curb, an accident, or modifying the height of your vehicle. When our car is out of alignment, our tires experience uneven “wear and tear” from shearing forces with the pavement that are not intended in certain areas on the tire. All of a sudden, the thick tread is diminished and you have to stop quickly in the middle of a snow storm. Excessive (deceleration) force + poor alignment + wear and tear = disaster. Yikes Momma. Does that clear things up?
Now that the physics is more clear, you may be asking yourself which one of the two scenarios is your problem. Are my quads tight and pulling my knee cap out of alignment? Or is it weak glute muscles causing my knee to collapse inwards creating a bad alignment at the knee joint? I am here to tell you it is both. You likely have tightness AND weakness. If this is depressing and baffling, then I am sorry because this is the truth and it is quite possible at this stage of your injury that: (sarah don’t do it).....
Please understand that this is a biomechanical downfall of almost every runner. Poor glute activation, weak/tight hips, terrible posture - it is not entirely your fault. Outside of our running endeavours, we are asked to work 40 hours/week (or more) while in a stationary position (sitting or standing) without encouragement to take stretching breaks or check our posture. Then, we are tired and go home to rest on the couch, read a book, or again - do something stationary. Being stationary can be a great thing! Especially if it involves engaging in stress relieving activities. And don’t get it twisted - your fellow physical therapists are also spending time in a stationary position with their legs crossed and hunched upper backs. We are told millions of things through the lovely avenue of social media that we “must do,” or “can’t miss,” for example:
Get 8-9 hours of sleep.
Meditate for at least 10-15 minutes.
Watch this season of The Bachelor.
Shape your eyebrows.
Eat less “junk food” and try the Keto Diet.
What a great list! Except number 5, I have a special place in my heart for chips and ice cream and refuse to label it as junk. That said, doing all of these things ON TOP OF taking care of our families, grocery shopping, laundry, cleaning, and exercise makes me want to sit on the couch just thinking about it. Twenty four hours sounds like plenty of time, but it is not always enough. Because guess what - you still haven’t foam rolled your quads, stretched your hip flexors, or strengthened your glutes yet. But you will do that “later” because you HAVE to squeeze in that 6 mile run according to your training plan.
What Are the Symptoms of Runner’s Knee?
This injury can be described in different ways depending if it is acute, chronic, level of severity, and/or the area that is experiencing the most irritation (i.e. tendon vs cartilage/bone, vs muscle). A newer, more acute injury will feel:
Sharp
Twingey
Nagging
“Nerve-y”
A more chronic injury will feel
Sore
Achey
Twingey
Stiff
Deep
Aggravating movements will include bending your knee, running, going down stairs more than going up stairs, jumping, deep squatting, or standing up from a seated position. You will find the knee to feel stiff after being sedentary or quite possibly first thing in the morning before you get out of bed.
Not all movement is irritating; though, as walking and gentle cycling can reduce the stiffness and make your pain subside. You will want to be careful with how much pain comes back after said activity, as this is the more telling factor. If you try running and your pain subsides, but you notice a return of symptoms and stiffness within a few hours after your run or even the next day, then running is definitely aggravating things. Could I be more of a joy-kill? Ugh #bearerofbadnews
What Activities Can You Do with Runner’s Knee?
Talk with your physical therapist or other healthcare provider, as sometimes running while having symptoms is okay. Most likely; though, you will be taking a break from running to focus on the factors that lead to this injury (see “How does this happen” above). I know I just talked about how your 24-hour schedule is already packed with chores, sleep, work, family, exercise, rest, and social activities. However, our lives are not defined by what we can fit into 24 hours. Instead, remember that you have more time than that - you have daily, weekly, monthly, and yearly routines to help spread out the tasks and make life more manageable. Afterall, running is a full time job. Not only do you have to run, but you also need to strengthen your muscles, stretch, work on mobility, foam roll, re-fuel, etc. But no one expects you to do these things everyday, nor should you. Everyone takes a “rest day.” So, start small by adding 15 minutes of stretching on your rest day. Even if that is through yoga, foam rolling, whatever - you choose what works best. Once that habit sticks, maybe you lengthen that to 30 minutes. Or, maybe you do 15 minutes of stretching and 15 minutes of glute exercises. Starting with 1 day/week sounds much less daunting and more doable than thinking you have to do all of these things everyday. Before you know it, you will find a routine that allows for working, running, childcare, laundry, foam rolling your calves, and doing your PT exercises.
As always - you can ice your knee after activity to reduce your pain, experience an epsom salt bath, use CBD creams for pain relief and reducing inflammation, and cross training on a bike, hiking, swimming, etc. in order to maintain cardiovascular fitness without engaging in an aggravating activity. Did I hear someone say aqua-jogging?
Last thing you can do is consider your shoes. Are your shoes older and worn down? Did you just buy new shoes and not adjust your training? If you struggle with chronic knee issues, maybe it is time to lower the drop on them bad boys. Having a lower drop reduces the compression forces on our knee caps by transitioning the load to our calves (be careful - we don’t want to trade patellar tendon injuries with achilles injuries). Discuss this with your physical therapist as shoes can make a big difference to our mechanics and force transmission.
How Long Does Runner’s Knee Take to Heal??
Well the classic, short, dreaded, but incredibly true answer is, “It Depends….”
So, giving you an exact prognosis is not fair to you or me, but in general this injury should resolve within 6-8 weeks assuming focus is placed on correcting the patellar tracking, increasing glute strength, improving joint mobility, and improving single leg mechanics through exercise and hands-on treatment. You will not need to remove yourself from running for the entirety of these weeks, and you may even be pain free within the first 2 weeks! But do not expect for things to be 100% resolved and fixed in those 8 weeks. You will improve so many aspects of your form and the health of your tissues from the knowledge and strength you will gain; however, don’t stop there. Maintaining strength and proper mechanics takes constant focus and reminders. It takes way less time to lose those skills and motor patterns than it does to build them, and we lose them by stopping the wonderful habits we learned from PT during the healing process. Keep strengthening your glutes, keep foam rolling after runs, keep doing mobility exercises, and keep addressing your posture. Your body will thank you down the road. Literally.
Helpful Exercises and Stretches for Runner’s Knee:
Clamshells
Bridges with ball squeeze
Single Leg bridges
Donkey kicks (band or no band)
Side steps and Monster Walks
Single leg mini squats
Single Leg RDLs
Couch/quad stretch
Planks
REFERENCES
1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5095937/
2.https://www.hopkinsmedicine.org/health/conditions-and-diseases/patellofemoral-pain-syndrome-runners-knee
3. https://www.runnersworld.com/health-injuries/a19578964/patellofemoral-pain-syndrome/
4. https://www.physio-pedia.com/Patellofemoral_Pain_Syndrome